
Pictured above is a surgeon viewing a CT scan for guidance while inserting a catheter. The x-ray is displayed at the patient’s bedside on a monitor. Developers hope to use Virtual Reality (VR) to virtually display a CT scan or x-ray, both for training purposes and to replace the monitor allowing easier viewing during surgery.
Virtual Reality (VR) has shown promise in displaying complex images in an immersive way. The Army, Air Force, and various police departments across the U.S. use VR to create training programs for specialized scenarios. Even businesses like Walmart and UPS are using VR to train employees on customer service, delivery routes and special safety circumstances. VR will revolutionize safety training, especially in industries where workers face a variety of scenarios. For this reason, medicine is one of the most important fields to integrate this technology. Medical staff from nurses to surgeons could train virtually to handle the pace, pressure and complexity of procedures.
The best application of VR in medical training is visualizing parts that may be too small or complex to view without using a microscope or cadaver. Systems like the central nervous or cardiovascular are impossible to view in a fully immersive way. Thus, VR makes the human anatomy much easier to study and less prone to error. CT scans, when viewed in an immersive virtual experience, further extend the specialist’s confidence and familiarity with the patient’s anatomy. In the same light, increasing the confidence level of practitioners has a positive effect on diagnosis and surgery prep. While common surgeries may not see immediate benefit, VR has larger implications for the most complicated and risky operations.
Virtual reality in aneurysm and coronary operations:
VR training is good for practicing highly precise surgeries, like on tiny arteries where a minor slip could be fatal. Surgeries dealing with artery aneurisms require heavy preparation specific to each patient’s anatomy. Virtual reality plays a vital role in the planning process, as surgeons can generate and inspect a recreation of the artery’s structure. Practitioners not only see but interact with the patient’s artery, identifying inflow and outflow arteries in a virtual setting. This makes all the difference in communication between radiologists, surgeons, other medical staff and the patient.
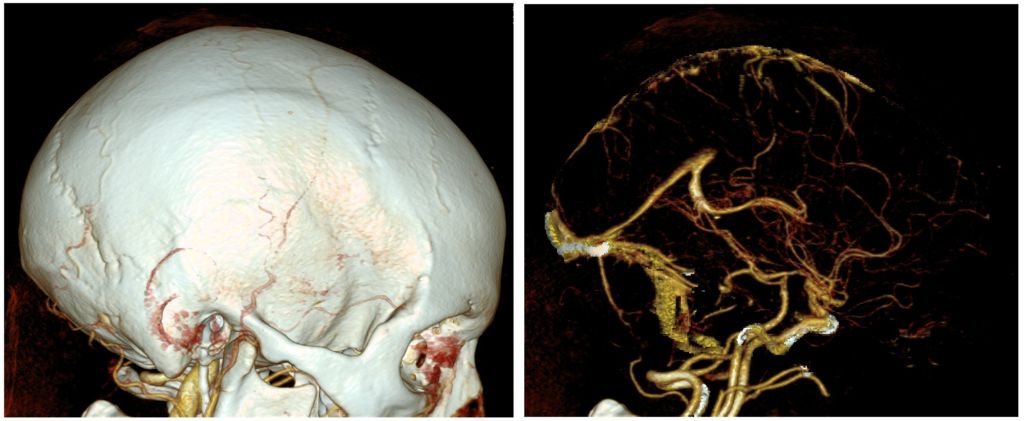
The photo above is a CT angiography (focusing on arteries) study on a human brain. These studies are extremely helpful when treating aneurysms and heart problems. With VR, practitioners can inspect and manipulate these scans in 3D before performing the operation in real time.
Cardiac radiologists have actively used VR in assisting with imaging, in one of the riskiest surgeries: coronary intervention. Full blockage of the coronary arteries is a large hurdle for catheter-based treatments for many reasons. Conventional coronary imaging techniques do not provide a complete picture of blocked arteries, adding further uncertainty to already unpredictable success rates. Surgeons from the Institute of Cardiology in Warsaw were able to use Google Glass to assist in coronary intervention. Normally, surgeons view CT scans on monitors alongside the operating table. Using a VR headset allowed the surgeons to see a 3D representation of the coronary artery without looking away from the patient.
This improves the surgeon’s guidance and operating efficiency, but also bypasses the cost of full CT suites and monitors. Mobile technology is experiencing heavy cost reductions, and is much more accessible than CT tech. As VR becomes proven in surgical use, mobile technology like glasses or headsets could bypass CT-monitor systems altogether.
VR in eye surgeries and diagnosis:
Optic nerves are difficult to study due to their size, as well as the delicacy of the human eye. Ophthalmology (the study of vision disorders) was advanced by leaps and bounds with the OCT scan, but they are far from perfect. It has become a common diagnostic method, but in its increased use, more and more errors are emerging. OCT scans are prone to false positives and negatives, where the color code of the scan is “tricked”. Red and Green are indicators of abnormal or normal tissue. Cases of severe nearsightedness sometimes throw off the OCT, which then shows opposite readings. User errors involving the setup of the OCT machine, or the patient’s head placement during the scan can also influence the outcomes of OCT studies.
A new virtual reality program enables OCT viewing with a retail VR device like the HTC Vive. Ophthalmologists can view and manipulate the OCT volume in 3D and can move it to any angle or position. In addition, they can draw markers along the OCT volume that indicate different segments of the eye (called “sectioning”). Some new research on sectioning focuses on using machine learning, but in surgery direct imaging displays trump automated methods. Visualizing the sectioning process lets ophthalmologists prepare for surgery by interacting with a lifelike recreation of the patient’s condition. Similarly. they could reduce the false results that plague OCT scans through more in-depth analysis. Researchers using a VR viewing tool can catch these errors before they lead to misdiagnosis or mistreatment.
The creators of this VR OCT viewer also tested the program for use in a simulated surgery. The VR tool was used in lieu of a microscope, as the surgeon could use the 3D display to navigate the optic structures. An assistant was needed to control the OCT scan so that the surgeon’s hands were free to operate. However, the process proved to be more effective as the surgeon did not need to stop and reference the OCTs for information. The VR headset is much less cumbersome than operating through a microscope and allows for better guidance with a live comparison of OCT volumes. This makes the procedure a more fluid and comfortable experience for the surgeon which will likely help improve outcomes.
Conclusion
VR technology, often associated with entertainment, has made remarkable strides in the medical field, particularly in enhancing complex, high-risk surgical procedures. The integration of VR in surgery offers improved navigational guidance and a more intuitive interface for surgeons, thereby increasing the precision and safety of operations. The ongoing research and development efforts aim to make VR technology more cost-effective, with a goal to significantly reduce the price of VR headsets for consumer accessibility.
Moreover, the potential of mobile VR technology is especially significant in developing markets, where the infrastructure for advanced medical imaging, like CT scans, may not be as prevalent. By making VR-assisted medical technologies more affordable, there’s a substantial opportunity to expand the accessibility of cutting-edge surgical and diagnostic procedures.
The broader adoption of medical VR could lead to more widespread preventative care, particularly for cardiovascular diseases, which are among the leading causes of mortality worldwide. The ability to utilize VR for enhanced visualization and training in CT technology can greatly improve the quality of care for heart-related conditions, making high-quality medical imaging and surgical precision more universally available.
As VR technology continues to evolve and become more integrated into medical practices, it holds the promise of democratizing access to advanced medical care, thereby improving health outcomes on a global scale. For an in-depth exploration of the latest advancements in VR and its transformative impact on various fields, including medicine, visit our recent article on Apple VR Headset.
References
- Dave Muoio. (2018) “Standford Study Finds Vr Imaging Boosts Radiologists Confidence”. MOBI Health News. Accessed on: https://www.mobihealthnews.com/content/stanford-study-finds-vr-imaging-boosts-radiologists-confidence
- Elsevier. (2015) “First In-man Use of Virtual Reality Imaging in Cardiac Cath Lab to Treat Blocked Coronary Artery”. Elsevier Research and Journals. Accessed on: https://www.elsevier.com/about/press-releases/research-and-journals/first-in-man-use-of-virtual-reality-imaging-in-cardiac-cath-lab-to-treat-blocked-coronary-artery
- Sanjay G. Asrani (2013) “OCT and Glaucoma: Artifact Alert”. Review of Ophthalmology. Accessed on: https://www.reviewofophthalmology.com/article/oct-and-glaucoma-artifact-alert
- Mark Draelos, Brenton Keller, Christian Viehland, Oscar M. Carrasco-Zevallos, Anthony Kuo, and Joseph Izatt. (2018) “Real-time visualization and interaction with static and live optical coherence tomography volumes in immersive virtual reality”. OSA Pusblishing, Biomedical Optics Express. Accessed on: https://www.osapublishing.org/boe/abstract.cfm?uri=boe-9-6-2825&origin=search